

Files
Download Full Text (799 KB)
Program
Emergency Medicine
Training Level
Resident PGY 1
Institution
Henry Ford Macomb
Abstract
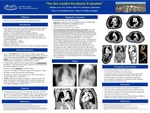
Aortic dissection occurs after a tear in the intima allows blood to enter the media and dissect between the intimal and adventitial layers, creating a false lumen which may extend anterograde or retrograde - Incidence: 2.6-3.5 per 100,000 person, bimodal age distribution - Risk factors: long-term HTN or connective tissue disorders (most common), preexisting aneurysm, bicuspid aortic valve, aortic coarctation, cocaine use - Classic presentation: tearing/ripping sensation, severe pain, pulse deficit, aortic regurgitation, tamponade -Painless dissection has been reported, although relatively uncommon (6.4% in one retrospective study) -Type A: ascending aorta – surgical tx -Type B: descending aorta – medical tx -Dx: CT w/ contrast -Acute Tx: reduce RATE first, then lower BP - Esmolol or Labetalol, Nitroprusside
Presentation Date
5-2019
Recommended Citation
Mikhjian, Gary and Francis, Omar, "Case Study: Type B Aortic Dissection in a Petitioned Patient (SI)" (2019). Case Reports. 110.
https://scholarlycommons.henryford.com/merf2019caserpt/110
