

Files
Download Full Text (572 KB)
Program
Dermatology
Training Level
Resident PGY 3
Institution
Henry Ford Hospital
Abstract
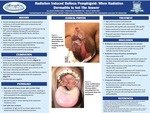
History: A 78-year old black female with history of invasive ductal carcinoma in the left breast status post lumpectomy and cytotoxic chemotherapy presented with acute onset blistering of the left breast with onset during the 24th cycle of radiation therapy which was diagnosed as radiation dermatitis by her radiation oncologist. New bullae on the left breast continued to arise after cessation of radiation therapy (RT). Within 4 weeks, patient was hospitalized with dysphagia, odynophagia, and oral ulcerations. At 8 weeks, patient developed new tense bullae on extremities and presented to dermatology. Examination: The entirety of the left breast extending onto the left flank had multiple flaccid serosanguinous filled bullae and erosions interspersed by well-demarcated depigmented patches with perifollicular macules of re-pigmentation. Three tense serosanguinous bullae were present on the right medial thigh, right medial lower leg and left calcaneal area. Two linear erythematous erosions with mild fibrinous debris extended from the hard palate down the oropharynx. Nikolsky sign was negative. There was no involvement of ocular or genital mucosa.Course and therapy: Punch biopsy of a bulla on the right medial thigh revealed subepidermal blisters with sparse infiltrate of lymphocytes and eosinophils in the underlying dermis. Direct immunofluorescence revealed 3+ linear IgG and C3 staining at the basement membrane zone. Salt split skin analysis revealed localization of linear IgG and C3 to the epidermal side of the dermal-epidermal junction, confirming the diagnosis of bullous pemphigoid (BP). Patient was treated with oral prednisone taper, high potency topical corticosteroids, and doxycycline 100 mg BID with niacinamide 500 mg BID in order to avoid immunosuppression.Discussion: Radiation dermatitis is a common cutaneous side effect of RT; however, persistent bullous eruption with spreads outside the radiation field requires further workup. BP is a rare complication of RT most often seen in breast cancer patients, but may occur in carcinomas of the lung, vulva, or esophagus. Etiology is unclear but may involve RT altering the basal membrane and expression of a mixture of hemidesmosome phenotypes by malignant breast cells which would serve as an antigen for antibody production inducing BP. The majority of cases occur during or up to 6 months after RT and tend to remain localized to RT-treated areas; rarely is there involvement of the oral mucosa. RT-associated BP appears more indolent than traditional BP and may respond to topical and non-systemic corticosteroid use.
Presentation Date
5-2019
Recommended Citation
Zarbo, Allison; Dunaway, Spencer; and Kerr, Holly, "Radiation Induced Bullous Pemphigoid: When Radiation Dermatitis Is Not The Answer" (2019). Case Reports. 30.
https://scholarlycommons.henryford.com/merf2019caserpt/30
