

Files
Download Full Text (661 KB)
Program
Cardiovascular Disease
Training Level
Fellow
Institution
Henry Ford Hospital
Abstract
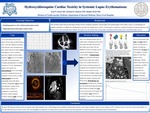
Learning objectives: Diagnosing and identifying patients at risk of developing Hydroxychloroquine cardiac toxicity. Introduction: Hydroxychloroquine (HCQ) and Chloroquine (CQ) were initially intended to be used as antimalarial drugs and are still prescribed for prophylaxis and treatment of malaria. Their effectiveness in rheumatoid arthritis and systemic lupus erythematosus (SLE) was found serendipitously and they have now become mainstays in the treatment of many connective tissue diseases. Prior literature details HCQ toxicities including retinopathy, neuromyopathy and cardiomyopathy. HCQ cardiac toxicity is an underdiagnosed condition and failure to withdraw the offending drug can lead to preventable adverse effects. A strong index of suspicion is required for patients on long-term therapy with HCQ to prevent this potentially fatal condition. We report a case of a patient with SLE found to have early HCQ cardiac toxicity. Case description: 59 year old female with a 30 year history of SLE stable on HCQ 200 mg twice a day since diagnosis presented with sub-acute onset of atypical chest pain. Initial work-up revealed an ECG with biphasic T waves in leads V3-V6 and a slightly elevated cardiac troponin I (cTnI) level of 0.16 ng/ml, with serial measurements in 3-5 hour intervals revealing levels at 0.14 ng/ml and 0.15 ng/ml, respectively (>0.04 ng/ml consistent with myocardial injury). Creatinine phosphokinase was mildly elevated at 275 IU/L. Inflammatory markers were normal. An echocardiogram (TTE) was normal except for a significant increase in estimated LV mass of 205 g, indexed at 130 g/m2. Cardiac catheterization and coronary angiography along with optical coherence tomography showed non-obstructive coronary artery disease and no evidence of spontaneous coronary artery dissection. Cardiac magnetic resonance imaging (cMR) was done to evaluate for myocarditis which was unremarkable. Chest pain persisted along with mild cTnI elevation upon follow up in clinic and she also admitted to slowly worsening exercise capacity and strength for the past several months. A skeletal muscle biopsy was performed showing myopathic changes and several collections of curvilinear bodies surrounded by lysosomal type membrane, largely consistent with HCQ toxicity. HCQ therapy was discontinued. On follow up ~4 months later, she denied chest pain and reported improvement in strength. Her cTnI level was decreased to 0.07 ng/ml. ECG was unchanged. TTE showed an estimated LV mass of 165 g, indexed at 105 g/m2, decreased from prior. Discussion: This is a report of HCQ-induced cardiac toxicity diagnosed via peripheral skeletal muscle biopsy in the setting of: biphasic anterior T wave changes on ECG; mild elevation of cTnI levels; and no abnormalities on TTE and cMR other than elevated LV mass. Our case demonstrates that ECG and cTnI might be useful screening tools to be used on a routine basis in patients on long-term HCQ therapy. LV mass on TTE might also be a sensitive marker of a sub-clinical histological process indicative of early HCQ-cardiac toxicity. Additionally, with the clinical context taken into consideration, an EMB can be forgoed by pursuing other less invasive tissue-organ biopsies if clinically suspected to be involved. Our patient’s cTnI level and LV mass on TTE improved several months after discontinuing HCQ which could be potential non-invasive follow-up markers used to assess outcome after drug withdrawal. Our patient did not have the misfortune of presenting with advanced heart failure or evidence of myocardial scarring due to early recognition and diagnosis. This report further highlights the importance of routine follow-up and screening along with a high index of suspicion in patients undergoing long-term HCQ/CQ therapy.
Presentation Date
5-2019
Recommended Citation
Isseh, Iyad; Hudson, Michael; and Modi, Shalini, "Hydroxychloroquine Cardiac Toxicity in a Systemic Lupus Erythematosus Patient" (2019). MERF 2019 - Case Reports. 5.
https://scholarlycommons.henryford.com/merf2019caserpt/5
