

Files
Download Full Text (612 KB)
Program
Orthopedic Surgery
Training Level
Resident PGY 2
Institution
Henry Ford Hospital
Abstract
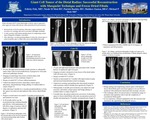
Purpose: Giant cell tumor (GCT) of the distal radius often exhibits a more aggressive disease course with increased rates of local recurrence and subsequent increased need for resection over curettage. In cases where resection of the distal radius becomes necessary, a variety of reconstructive techniques exist without notable clear superiority of any one. Presented here is a small series of GCT of the distal radius treated with resection of distal radius, temporizing cement spacer (Masquelet technique) and bridge plating. After formation of a pseudomembrane, the cement spacer was removed and a freeze-dried fibula graft was implanted with good clinical and oncological outcome.Materials/ Methods: Case 1: 64 year old right hand dominant female presents with several month history of progressive wrist pain and associated recent pathologic fracture. Imaging revealed large lytic lesion of distal radius with significant loss of bone continuity. Biopsy revealed GCT of bone without metastases and the patient underwent radical resection, intercalary cement spacer placement, and preliminary bridge plating of residual radius to carpus. After allowing 6 months for a vascular pseudomembrane to form, the spacer was removed and replaced with a freeze-dried fibular graft. Progress toward union was noted 4 -5 months postoperatively and matured over time. At 48 months follow up, the reconstruction has remained durable and effective with maintenance of full elbow range of motion, with 45 degrees of supination and near full pronation.Case 2: 37 year old right hand-dominant male presented with 3 month history of significant right wrist pain. Imaging revealed a destructive bone lesion of the distal radius with soft tissue mass. Biopsy revealed GCT of bone and patient was placed on denosumab for 3 months with improvement in pain and increased mineralization noted on imaging. He then underwent curettage and grafting after the denosumab treatment. Questionable recurrence was noted at approximately 8 months post operatively. Two months later, the patient underwent wide resection, intercalary cement spacer and bridge plating of residual radius to carpus. Eight months later, the paitent underwent conversion of intercalary spacer to freeze-dried fibula with early incorporation noted at 6 months postoperatively. Patient maintained full elbow ROM with 30-40 degrees of supination and full pronation.Discussion: Functional reconstruction after distal radius resection is challenging. A novel and straightforward technique allowing for preservation of satisfactory range of pronation and supination is presented. This technique avoids the complexity of vascularized fibula grafts. In addition, delayed implantation into the resection bed maximizes the opportunity for allograft success. Conclusion: Bridge plating and temporizing cement spacer with delayed freeze-dried fibula graft conversion appears to be an effective treatment with satisfactory functional and oncologic outcome.
Presentation Date
5-2019
Recommended Citation
Fisk, Felicity E.; Mott, Nicole; Buckley, Patrick; Easton, Matthew; and Mott, Michael, "Giant Cell Tumor of the Distal Radius: Reconstruction with Masquelet Technique and Freeze Dried Fibula" (2019). MERF 2019 - Case Reports. 69.
https://scholarlycommons.henryford.com/merf2019caserpt/69
