

Files
Download Full Text (1.1 MB)
Program
Dermatology
Training Level
Resident PGY 4
Institution
Henry Ford Hospital
Abstract
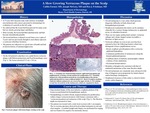
A 73 year-old Caucasian male with a history of multiple non-melanoma skin cancers presented to dermatology for evaluation of a growth on the left scalp. He endorsed that the lesion had been present for many years but was slowly growing larger and thicker and had recently bled spontaneously and become intermittently painful. The lesion had been evaluated several times over a span of 3 years and was previously thought to most likely represent a verrucous seborrheic keratosis. The patient was otherwise in a good state of health and had no known history of immunosuppression.On the left parietal scalp there was a pink-brown verrucous plaque with filiform projections and focal hemorrhagic crust. The lesion measured 5.2 cm x 3.8 cm.Saucerization biopsy of the most exophytic portion of the lesion was performed and revealed a broad, atypical melanocytic proliferation within a larger verrucous keratosis with features consistent with a ‘verrucous pseudonevoid melanoma of the scalp. The Breslow depth was measured at 1mm.The patient was treated with a wide local excision with 1 cm margins. The re-excision specimen showed focal residual melanoma in-situ and clear margins. A sentinel lymph node biopsy was performed for staging and was found to be negative for metastatic disease.Nevoid melanoma is a rare entity which presents diagnostic difficulty on both clinical and histopathological grounds. On physical examination this tumor can be mistaken clinically for a verruca, benign melanocytic or epidermal nevus, or seborrheic keratosis. There are two major architectural variants: verrucous subtype and a dome-shaped variant (resembles a Meissner or Spitz nevus). The verrucous-subtype (as seen in our case) has been reported to have the following features which may distinguish it from a papillomatous nevus: (1) broad, exophytic growth pattern with a verrucous epidermal hyperplasia, (2) continuous proliferation of melanocytes along the dermal-epidermal junction, (3) confluent sheets of uniform, monomorphic without evidence of true maturation, and (4) occasional dermal mitoses.Mortality related to nevoid melanomas is thought to be consistent with that of traditional melanomas of the same Breslow depth. However, nevoid melanomas are commonly more advanced at the time of diagnosis given propensity for initial clinical and/or histologic misdiagnosis. Therefore, heightened awareness of this entity is critical to better ensure earlier diagnosis.
Presentation Date
5-2019
Recommended Citation
Farmer, Caitlin; McGoey, Joseph; and Friedman, Ben J., "A Slow Growing Verrucous Plaque on the Scalp" (2019). MERF 2019 - Case Reports. 21.
https://scholarlycommons.henryford.com/merf2019caserpt/21
