

Files
Download Full Text (797 KB)
Program
Internal Medicine
Training Level
Resident PGY 1
Institution
Henry Ford Hospital
Abstract
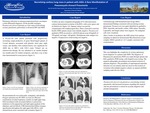
Introduction: Pulmonary infections in immunocompromised hosts encompass a wide differential diagnosis. Of the possible etiologies, Pneumocystis jirovecii presents as a rare cause of necrotizing cavitary pneumonia, particularly in patients with advanced HIV and AIDS. We present the case of a cavitating lung lesion in a patient with AIDS, as an example of this rare atypical manifestation of Pneumocystis, hoping to increase clinical awareness and assist in prompt diagnosis and management. Case: A 50-year-old male patient presented with progressively worsening cough productive of green blood-tinged sputum of 2-week duration, associated with pleuritic chest pain, night sweats, and diarrhea. Past medical history was significant for AIDS due to HIV-1 with CD-4 count 73/mm3 not on antiretroviral therapy. He was admitted to an outside hospital two months prior for similar symptoms, and chest x-ray at that time demonstrated no acute process (figure 1). On presentation he was tachycardic, tachypneic, and afebrile. Oxygen saturation was 98-100% on room air. Physical examination revealed inspiratory crackles on right upper lung field auscultation with associated dullness to percussion, tenderness in the epigastrium and right upper quadrant of the abdomen, and oral thrush. CXR demonstrated diffuse airspace opacification throughout the right upper lobe (RUL), with internal lucent areas consistent with cavitation (figure 2). A follow-up chest computed tomography (CT) with intravenous contrast demonstrated cavitation of the RUL, with cystic spaces and air fluid levels (figure 3,4). Sputum culture was grossly contaminated with oropharyngeal flora. Three consecutive acid-fast bacilli (AFB) sputum smears were initially negative. Pneumocystis qualitative PCR was positive, with B-D glucan assay (Fungitell) of 239 pg/mL (ref range: <60 pg/mL). Histoplasma urine antigen was negative. Cryptococcus serum testing was negative. A bronchoscopy with bronchoalveolar lavage (BAL) demonstrated findings consistent with necrotizing cavitary pneumonia. Pneumocystis was again identified on qualitative PCR. Anaerobic and aerobic culture, AFB culture, Nocardia, Legionella, and fungal culture were negative. No malignant cells were visualized. After 4 weeks of incubation, the AFB culture from sputum sampling on admission demonstrated Mycobacterium avium complex (MAC) growth in 1 of 3 samples consistent with contamination.Discussion: This case highlights the complexity of cavitary pulmonary lesion diagnosis in a patient with AIDS. The diagnosis of Pneumocystis pneumonia (PCP) was made through sputum and BAL qualitative PCR testing, with fungitell assay testing. The atypical radiographic presentation necessitated exclusion of alternate diagnoses. The possibility of superimposed anaerobic infection was not entirely ruled out, however the location of cavitation with multiple negative cultures on sputum and BAL sampling made this less likely.Conclusion: Pneumocystis jirovecii can present as a necrotizing cavitary pneumonia, and increased awareness regarding this atypical and rare presentation is critical for accurate diagnosis and prompt management.
Presentation Date
5-2019
Recommended Citation
Fadel, Raef; Ouellette, Daniel; Ramo, Aula; Binz, Sophia; and Abreu-Lanfranco, Odaliz, "Necrotizing Cavitary Lung Mass in Patient with AIDS: A Rare Manifestation of PCP" (2019). MERF 2019 - Case Reports. 48.
https://scholarlycommons.henryford.com/merf2019caserpt/48
